Reimagining treatment readiness
for oncology operations.
Lynx's highest-traffic Queue → Dispense workflow looked like a two-step modernization problem. Research showed something larger: oncology teams were using the Queue to coordinate treatment readiness work the product did not otherwise support. As research, strategy, and design lead, I reframed the effort from improving a transaction flow to shaping a readiness-driven decision-support workflow — helping users understand who is ready for dispense, what is blocked, what medication may be needed, and where human judgment is required.
Lynx was structured around transactions. Clinics were structured around treatment readiness.
Established treatment readiness as the first workflow modernization anchor for Lynx.
The work shifted the modernization direction from improving a high-traffic Queue → Dispense flow to supporting treatment readiness as the organizing model for future workflow design.
Six capabilities that moved from manual work to supported workflow
Readiness-driven dispense workflow
The concept moved away from manual Queue construction toward automatically surfacing who is ready for dispense, who is blocked, and what needs attention.
Medication demand forecasting
Helps inventory and ordering staff understand what high-cost medications may be needed before treatment day so practices can prepare without overstocking.
Vial optimization
The system recommends the optimal vial combination to minimize billable waste and cost. Users review, adjust, or override before ordering or dispense.
Role-aware workflow support
Separates planning decisions (inventory and ordering staff before treatment day) from point-of-care confirmation (dispensing staff at the cabinet).
Exception recovery
Dose changes, schedule changes, and readiness gaps are treated as expected workflow states — resolved in place rather than requiring users to delete and rebuild queued work.
Modernization foundation
Identified reusable patterns for readiness states, recommendation explanation, human review, and future AI-supported workflows across Lynx.
From Queue management to treatment readiness
Current workflow
Users manually prepare, queue, check, report, order, recover from changes, and dispense across Lynx and outside tools.
Future direction
Lynx surfaces readiness, medication demand, vial guidance, exception recovery, and human review before dispense.
A Workflow Connected to Physical Point-of-Care Operations
Lynx supports medication purchasing, inventory, and dispense workflows for oncology practices — connected to EHR systems, purchasing workflows, inventory data, and physical pharmacy cabinets. The workflow is not only digital: it affects what happens at point of care.
Inventory & ordering staff need to
- Know what high-cost medications to prepare before treatment day
- Estimate demand without over- or under-ordering
- Coordinate across sites and suppliers
Dispensing staff need to
- Confirm the right medication, dose, and vial configuration
- Verify cabinet access and physical inventory at point of care
- Resolve changes without rebuilding queued work
Treatment readiness sits between two risks: under-ordering means the patient arrives without the right drug on hand; over-ordering means the practice carries expensive inventory it can't use or bill for. The workflow had to help staff navigate that window every day.
System at a glance
People
Inventory and ordering staff · Infusion nurses · Pharmacy technicians · Remote coordinators · Account managers
Systems
Lynx · EHR · Customer Center · Cabinets · Reports · Spreadsheets
Core decisions
What to order · Who is ready · Which vials to use · What changed · When it is safe to dispense
Constraints
High-cost medications · Tight inventory margins · EHR variability · Day-of order visibility · Cabinet access · Human oversight
Expanding the workflow from dispense to readiness.
Queue and Dispense were the highest-traffic areas in Lynx — a clear starting point for modernization. The initial assumption: a two-step workflow problem. Research showed the real work started much earlier.
Before a single patient reached the Queue, staff were already:
- Reviewing future schedules and estimating medication demand
- Checking inventory and calculating vial combinations by hand
- Managing dose and schedule changes across multiple systems
- Coordinating between ordering, pharmacy, and infusion roles
- Reconciling information from EHRs, reports, spreadsheets, and memory
Lynx primarily supported the final transaction. Most of the readiness work happened outside the product.
When hours of preparation sit outside a two-minute dispense action, the opportunity is bigger than usability. It is the product boundary — and moving it meant redesigning how Lynx understood treatment readiness, not just how the Queue page looked.
1. Give readiness work a clear home
Treatment readiness includes confirming patients, orders, drugs, inventory, changes, and staff readiness. The opportunity was to support this daily preparation work directly in Lynx.
2. Separate planning from same-day dispense
The Queue was acting as a planning tool, demand signal, readiness monitor, exception recovery space, same-day execution list, and cabinet access trigger. The opportunity was to separate those jobs into clearer workflow moments.
3. Support high-stakes calculations
Vial selection, demand estimation, and cross-site inventory checks were performed by hand. These calculations affect cost, waste, purchasing, and clinical readiness every day.
4. Resolve changes without rebuilding work
Dose changes, schedule changes, and validation errors needed clearer recovery paths, so users could resolve changes in place instead of deleting and rebuilding queued work.
Understanding how people actually used Queue and Dispense
We used customer interviews, workflow discovery, journey mapping, SME conversations, usage signals, and concept validation to understand how people actually used one of the highest-traffic areas in Lynx. Each method revealed a different layer of the same finding: the real work started before the Queue, and most of it happened outside Lynx entirely.
Customer interviews and workflow discovery
Why this method: We needed to understand what users were trying to accomplish with Queue and Dispense, not just how the workflow was intended to work.
What it revealed: Users were relying on Queue and Dispense to manage broader treatment readiness work, including preparation, demand estimation, inventory checks, changes, and dispense coordination.
Journey and workflow mapping
Why this method: The work spanned multiple roles, systems, and time horizons, so we needed to map what happened before, during, and after dispense.
What it revealed: Treatment preparation began before the Queue step and often happened across EHRs, reports, spreadsheets, Customer Center, Lynx, and memory.
SME conversations
Why this method: We needed practice-level context around EHR integration, inventory constraints, medication ordering, and how different roles coordinate work.
What it revealed: The workflow had to support different customer setups, including practices where future order visibility is limited or unavailable.
Concept validation
Why this method: We needed to test whether a readiness-driven direction made sense before engineering commitment.
What it revealed: Internal reviewers needed visible reasoning, role-aware information density, clear override paths, and support for sites where future order visibility could not be assumed.
Anonymized journey map showing how treatment readiness work spans Lynx, EHRs, reports, spreadsheets, manual bridges, and pain points before and during dispense. Three participant contexts: Rheumatology/NextGen, Oncology/Varian, Oncology/iKnowMed G2.
From Queue modernization to a readiness-driven workflow.
Research started with one question: how should we modernize Queue → Dispense? It ended with a different one: how might Lynx support treatment readiness before users manually build a Queue?
- Queue and Dispense were being used to coordinate readiness work — not just complete transactions
- Users managed demand estimation, inventory checks, vial calculations, and change recovery in a tool not designed for any of it
- The Queue had become a manual planning layer for readiness work Lynx didn't otherwise support
That shifted direction from modernizing the Queue page to exploring a readiness-driven workflow — one where Lynx surfaces who is ready, what is blocked, what medication may be needed, and where human review is required.
Lynx was structured around transactions. Clinics were structured around readiness.
The current workflow made sense if the primary job was completing a dispense transaction. But clinical teams were solving a broader readiness problem before that transaction could happen.
What clinics need to answer before treatment
Exploring how far modernization needed to go
The ideation question changed as we learned more. At first: How might we improve the Queue → Dispense flow? After research and SME review: How might Lynx identify treatment readiness before users manually build a Queue?
Direction considered: Modernize the existing Queue page
What we learned: it could reduce friction in the current interface, but users would still have to manually determine who belonged in the Queue, what was missing, what needed to be ordered, and whether the patient was actually ready for dispense.
Direction considered: Add readiness indicators to the Queue
What we learned: it would improve visibility, but it would keep the Queue as the organizing model even though readiness work begins before a patient should be queued.
Direction chosen: Readiness-driven dispense workflow
The system should identify and surface readiness instead of making users manually construct a Queue. This better supports planning, medication availability, vial optimization, exception recovery, and point-of-care dispense.
Designing for real-world workflow variability
Readiness varies by customer setup: EHR integration, order visibility, scheduling data, and workflow constraints all affect what Lynx can know before treatment day. The design had to work across all of them.
- EHR integration ranges from fully integrated to manual-only — the workflow needed to function across all setups
- Order visibility varies — some practices see future orders days ahead, others only on the day of treatment
- Planning windows differ — advance ordering timelines vary by practice and location, requiring configurable preferences
- Multiple roles interact at different points: pharmacy operations, infusion nurses, pharmacy techs, remote coordinators
EHR integration variability
- Integration ranges from fully connected to manual-only
- Workflow needed to support all levels without degrading for less-integrated sites
Day-of order visibility
- Some practices only see orders in Lynx on the day of treatment
- Staff use forward schedule data to estimate demand manually
- Readiness support could not depend on confirmed orders alone
Multiple user roles
- Pharmacy operations, infusion nurses, pharmacy techs, and remote coordinators all interact with the same workflow
- Each role has different information needs and decision authority at different points
Physical cabinet dependency
- Dispense is tied to physical cabinet access — not purely a digital workflow
- Sequencing, confirmation, and recovery paths affect real point-of-care operations
Customer setup affects what Lynx can know before treatment day
Customer setup
Strong EHR integration
Day-of order visibility
Limited or no integration
What Lynx may know early
Schedule + orders
Schedule before orders
Manual inputs or reports
Design implication
Surface readiness earlier
Forecast with caveats
Support review and override
Making dispense readiness visible before treatment day
The design direction moved toward a readiness-driven workflow — automatically surfacing who is ready for dispense, what is blocked, what medication may be needed, and where human review is required.
The goal was not to automate clinical judgment. The goal was to reduce the manual coordination and calculation staff must do before they can make informed decisions. The system carries the work. Humans retain review, adjustment, and control.
Make readiness visible earlier
- Surfaces who is ready for dispense, who is blocked, and what is missing
- No manual Queue construction — readiness determined by the system
- Available before the patient arrives, not only at point of care
Automate advance ordering preparation
- Translates upcoming treatment demand into order-ready items
- Reduces manual burden: no more running reports and adding medications to cart by hand
- Staff retain review and approval before any order is placed
Recommend vial combinations with human review
- System calculates the optimal vial combination — users review, adjust, or override
- Reduces cognitive load and error risk on high-stakes, high-cost decisions
- Supports tighter inventory margins by minimizing billable waste
Separate planning from point-of-care confirmation
- Ordering staff work ahead of treatment day; dispensing staff confirm at the cabinet
- Each role sees the information density they need — not the same view forced on everyone
Support changes without rebuilding work
- Dose and schedule changes treated as expected states, not errors
- Resolved in place — no deleting and rebuilding queued work
Preserve human judgment and override
- System surfaces recommendations and reasoning — users decide
- Human approval required before ordering and before dispense
- The system carries the calculation. Humans retain control.
Future-state screens created in Figma Make and Replit to test workflow direction, reasoning visibility, and human review before engineering commitment.
1. Surface medication demand before treatment day
Readiness does not start at dispense. For inventory and ordering staff, the workflow begins days earlier with medication demand, inventory checks, and ordering preparation. The prototype explores how Lynx could surface upcoming demand and turn it into reviewable order actions before treatment day.
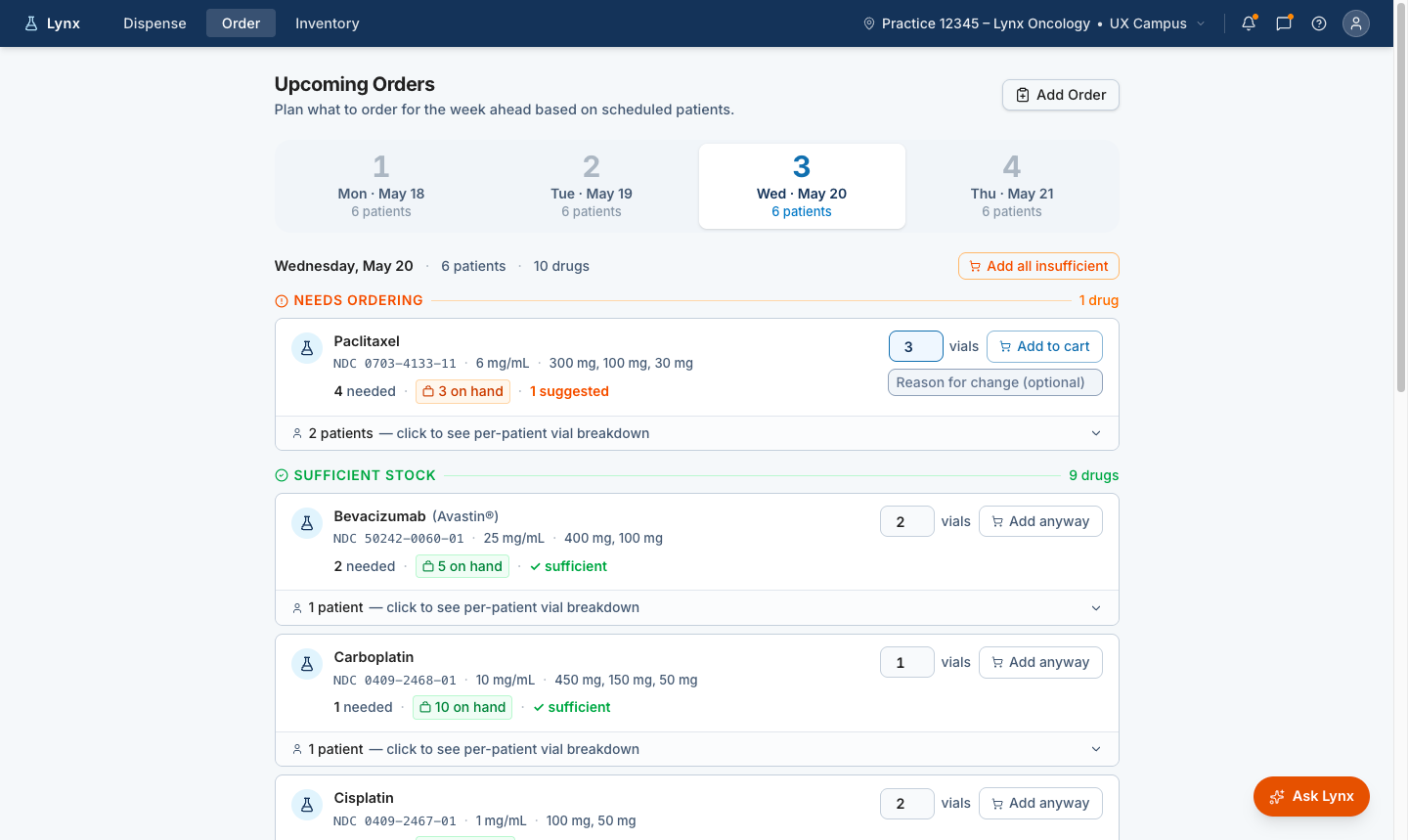
Future-state order planning view showing how Lynx could translate upcoming treatment demand into recommended order actions while keeping staff in control of review and cart decisions.
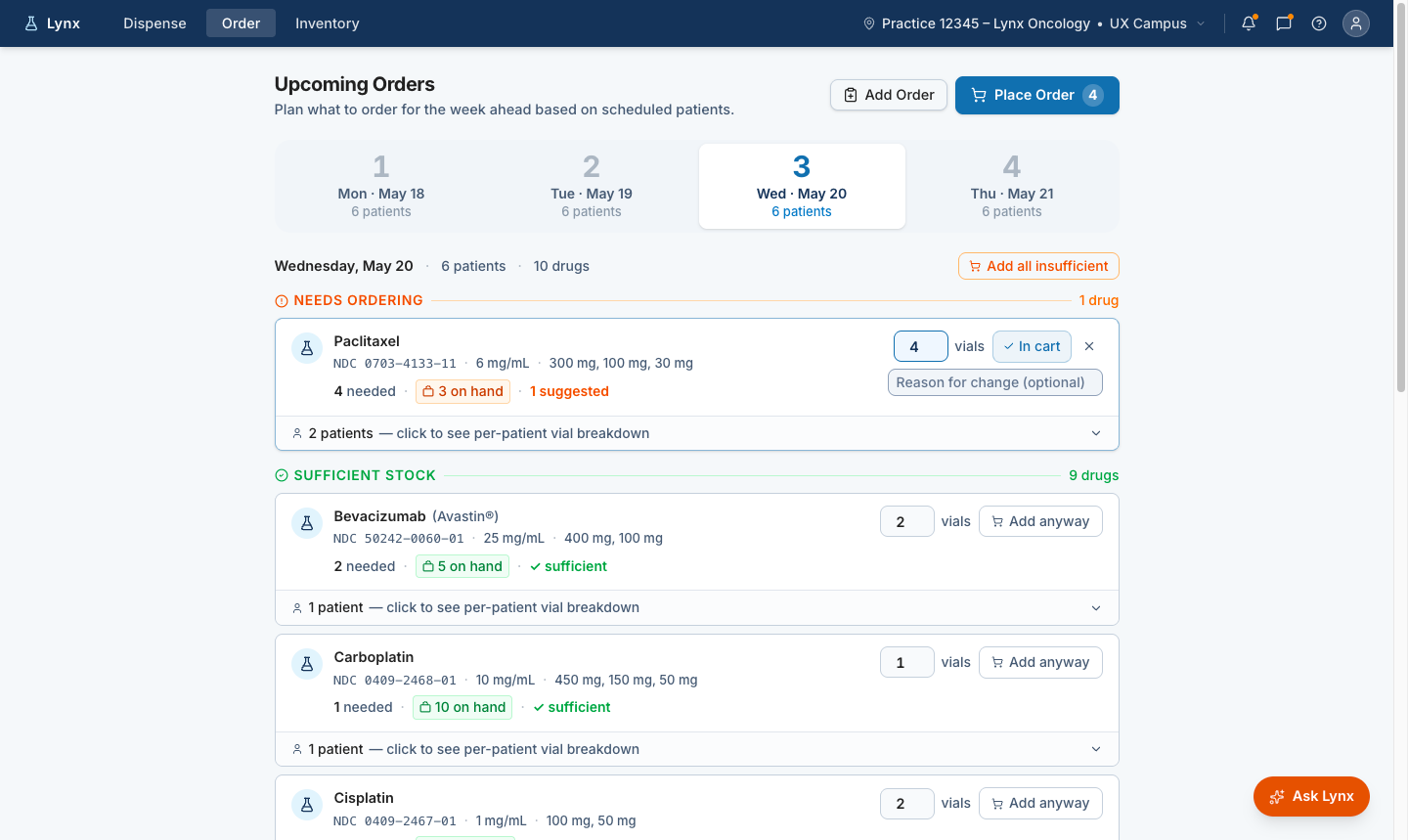
Reviewable cart action
Suggested quantities can be adjusted and added to the cart, keeping ordering staff in control before an order is placed.
Patient-level transparency
Staff can expand the recommendation to see the patient-level vial breakdown behind the suggested order quantity.
The recommended order flow keeps the user in control by showing suggested quantities, cart actions, and patient-level reasoning before order placement.
2. Show who is ready for dispense
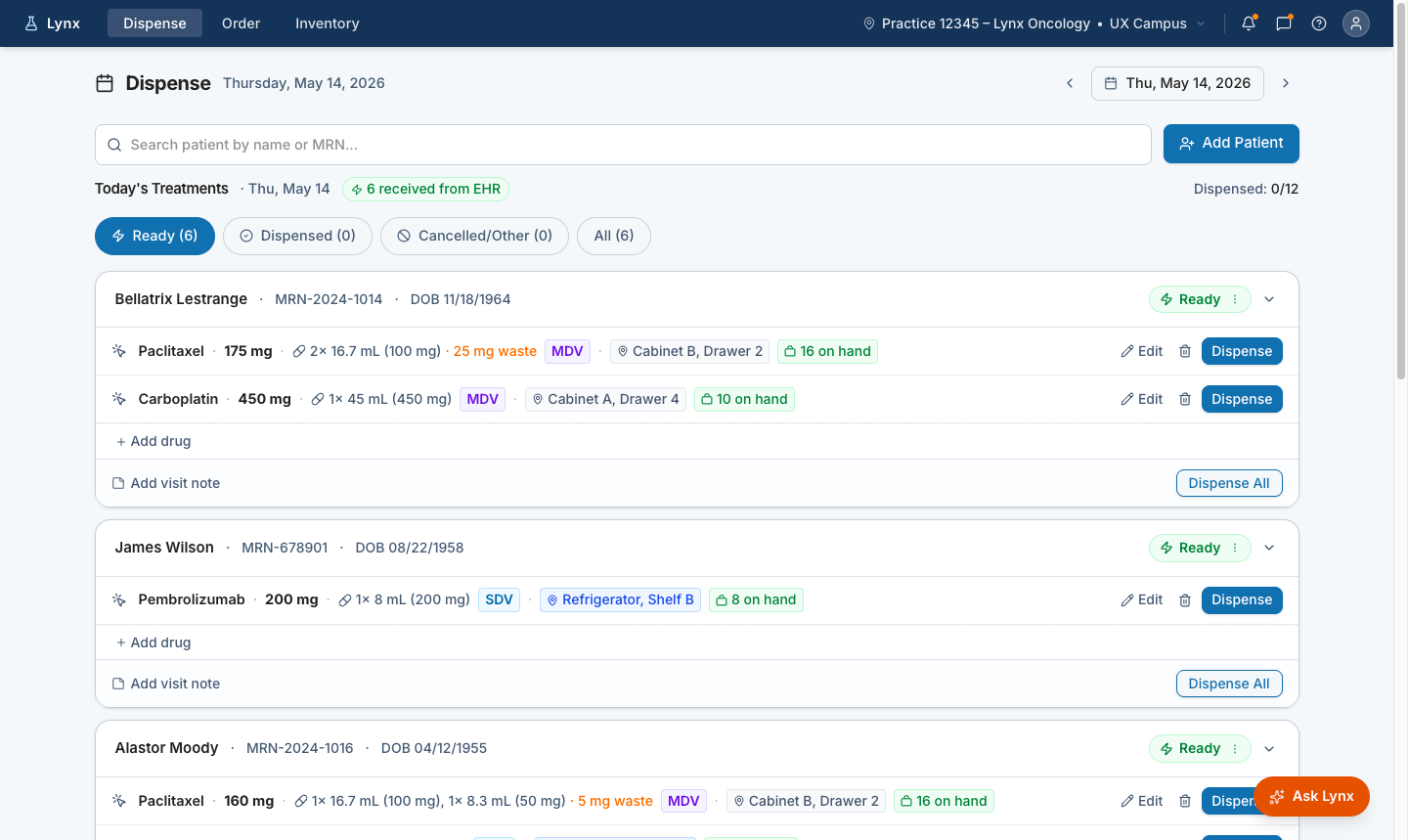
Future-state dispense view showing which patients are ready for treatment on the selected day, with medication, inventory, storage location, and dispense actions surfaced in one place.
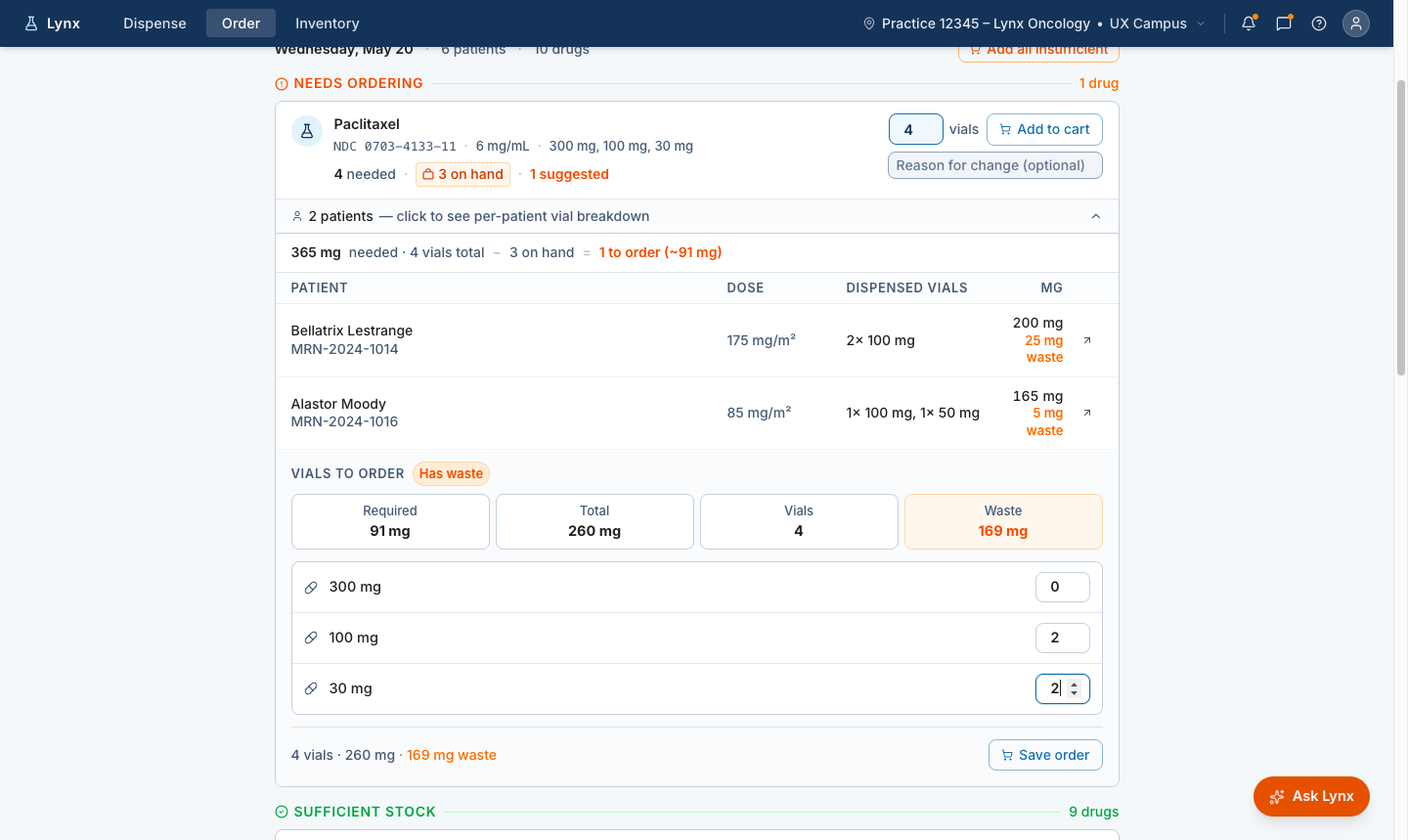
3. Recommend vial combinations with human review
For high-cost medications, vial selection is both an operational and financial decision. The prototype recommends an optimal vial combination, makes waste visible, and allows staff to adjust the recommendation when real-world conditions require it. The system carries the change forward so downstream users can see that the dispense work was adjusted.
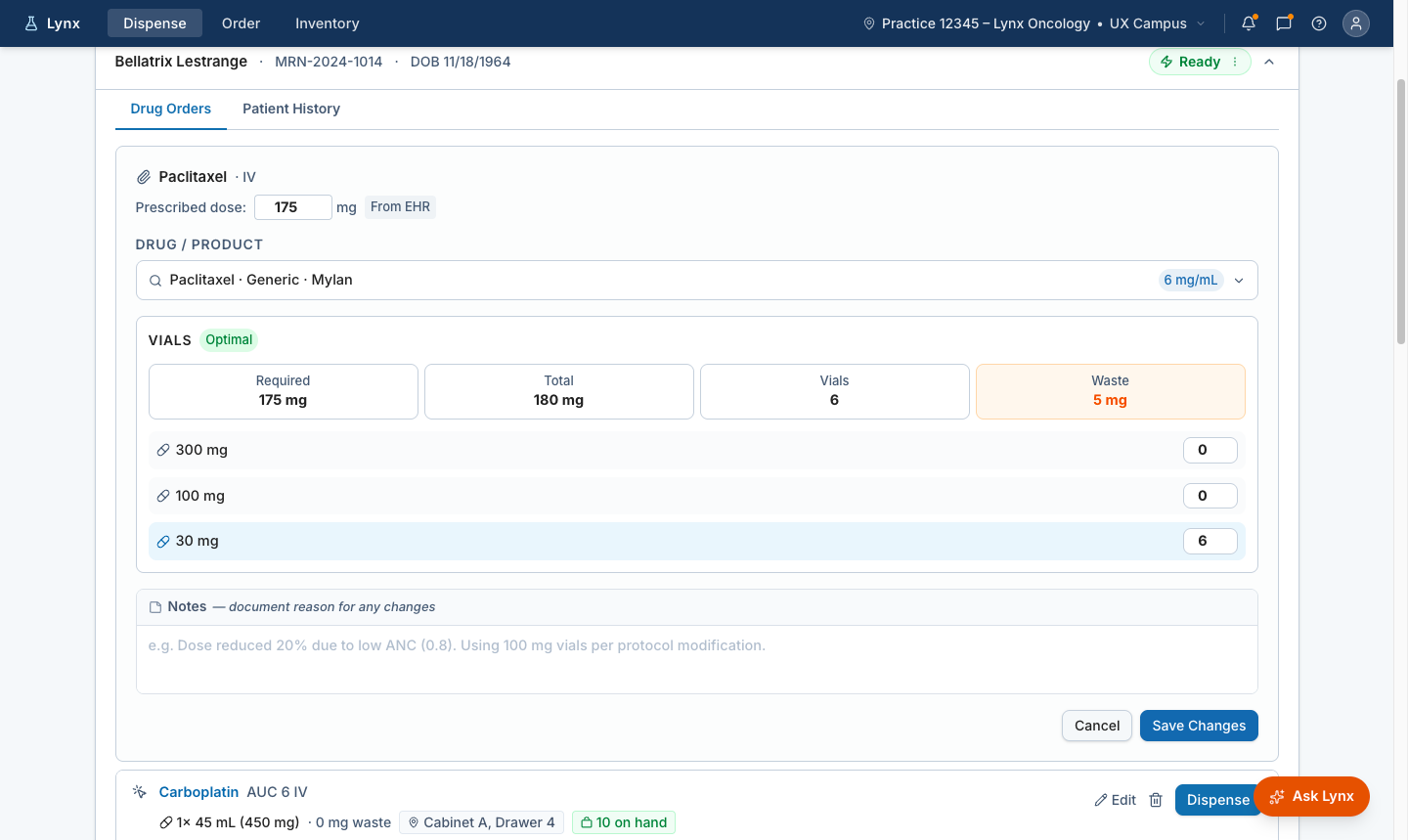
Lynx recommends an optimal vial combination for the prescribed dose, making total dose, vial count, and expected waste visible before dispense.
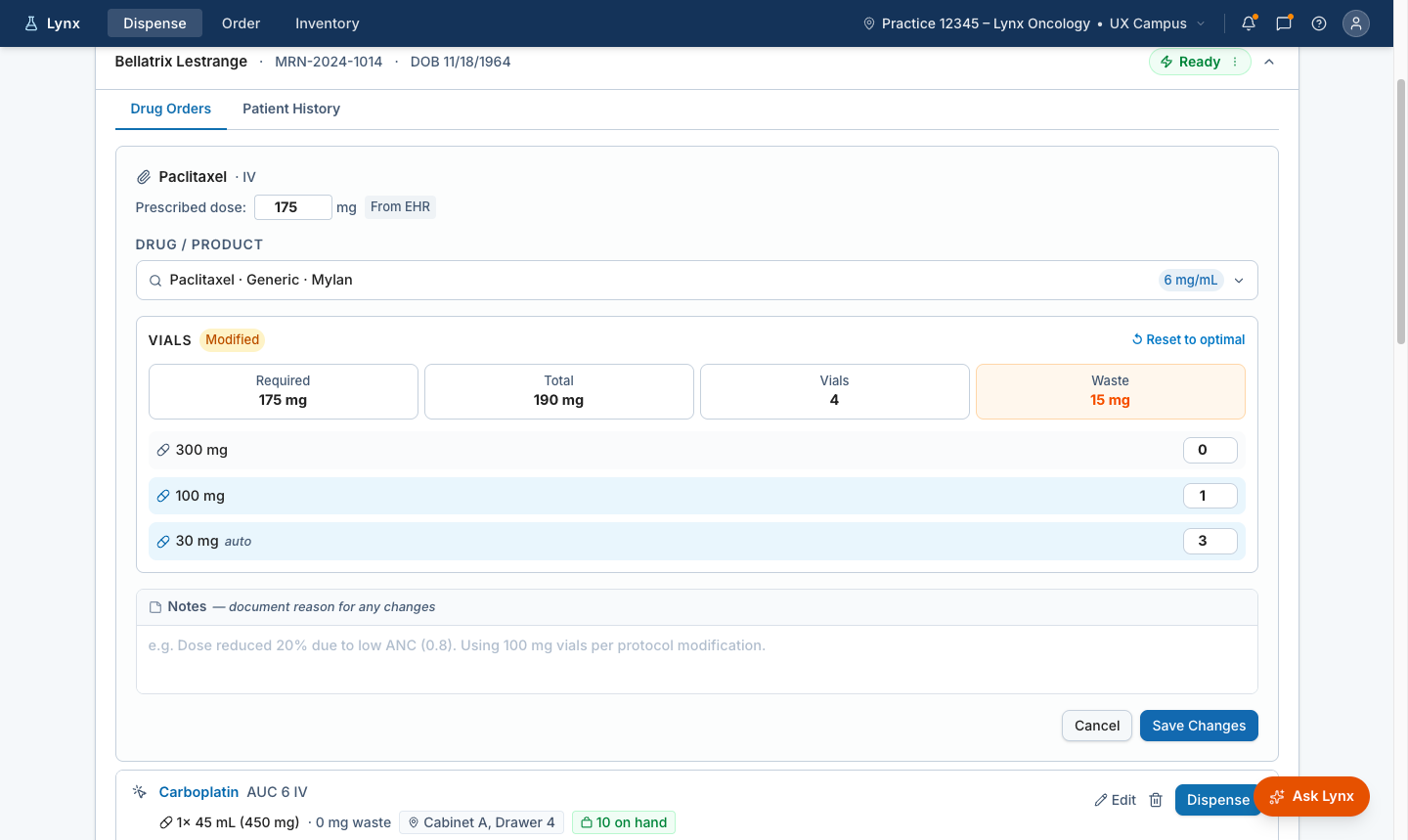
Override with recalculated waste
When staff change the recommended vial mix, Lynx recalculates total dose and waste immediately so the impact of the change is visible before saving.
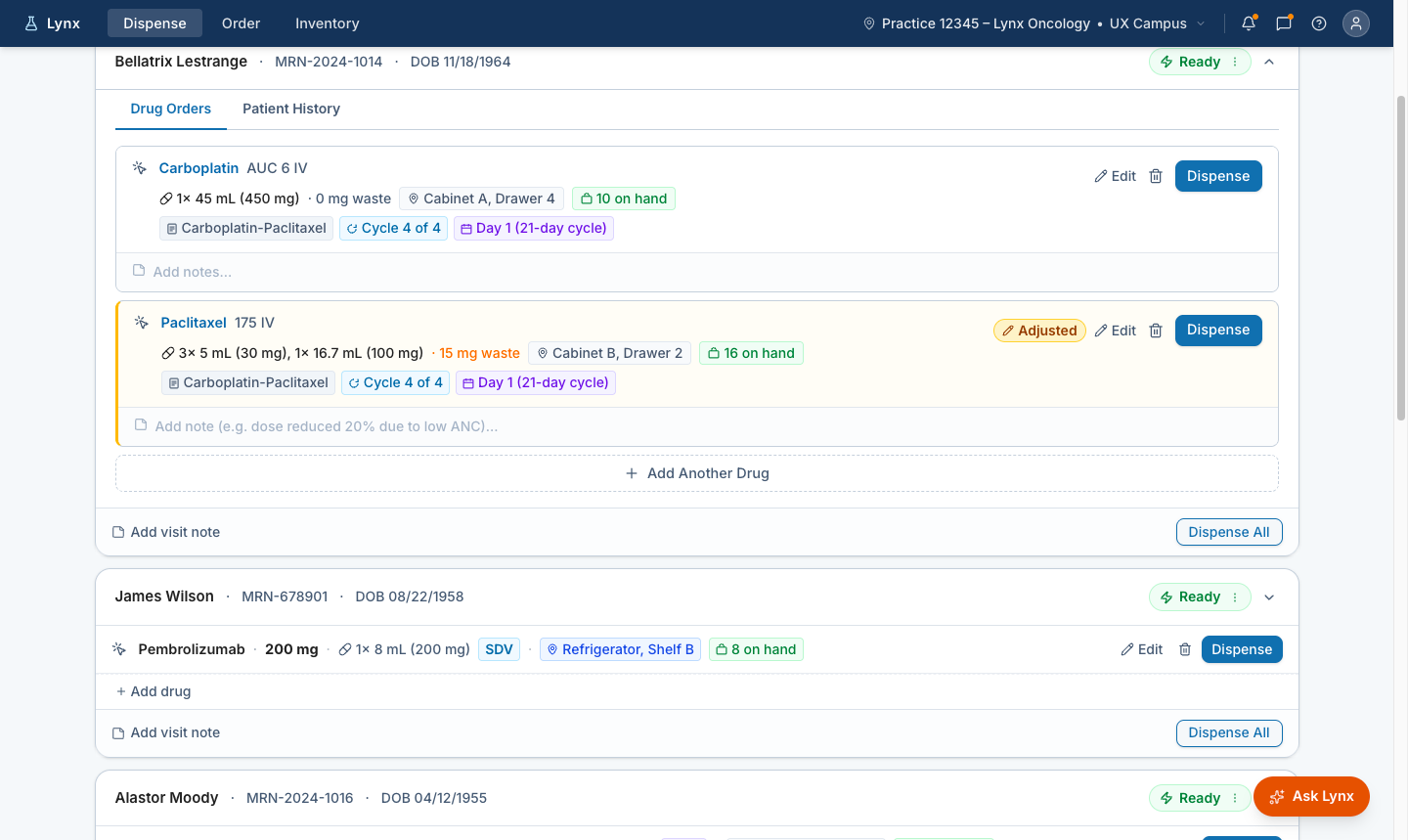
Adjusted state carried forward
The updated vial configuration carries into the dispense workflow with a clear adjusted state, so downstream users can see the recommendation changed.
When staff adjust the recommended vial mix, Lynx recalculates waste immediately and carries the change forward into the dispense workflow with a clear adjusted state.
Building confidence before customer validation
Because this work is pre-alpha, outcomes are framed as intended outcomes, validation questions, and future measurement areas rather than finalized performance results. The prototype was reviewed with Customer Success and Account Managers to understand whether the readiness model reflected practice workflows, where the concept needed clarification, and what questions should be taken into customer validation.
Internal review with Customer Success and Account Managers helped clarify where the readiness model aligned with practice workflows, where the concept needed refinement, and what questions to take into customer validation.
How the work shaped modernization beyond the prototype
Aligning Product, Engineering, Customer Success, Account Management, and UX around a shared problem definition before engineering commitment became part of the deliverable. It changed the conversation from what Queue should look like to what treatment readiness needed to become.
Product direction
- Established treatment readiness as the modernization anchor for Lynx
- Shifted the conversation from Queue cleanup to a readiness-driven workflow model
Information architecture
- Moved the team from legacy pages and reports to clearer workflow moments
- Planning · Readiness review · Medication demand · Vial guidance · Exception recovery · Dispense
Cross-functional alignment
- Product · Engineering · Customer Success · Account Management · UX
- Shared problem definition established before engineering commitment
Validation approach
- Live prototypes validated with Customer Success and Account Managers before customer sessions
- Concept direction confirmed before engineering commitment
Design system input
- Reusable patterns identified for: readiness states, recommendation explanation, human review, exception recovery
- Foundation for future AI-supported workflow patterns across Lynx
Operational workflow model
- Defined advance medication planning, ordering preparation, and dispense readiness as distinct workflow moments
- Helps teams design beyond the legacy Queue and account for how practices actually prepare treatment days
Related work — AI-Assisted Design Delivery Pipeline
The Treatment Readiness prototype informed the AI-assisted design delivery pipeline and the emerging Lynx design system, including reusable patterns for decision support, human review, and exception recovery. Building an AI-Assisted Design Delivery Pipeline →
Future direction — Ask Lynx
Ask Lynx builds on the same modernization direction: helping users find information, understand changes, recover from exceptions, and navigate complex workflows without replacing clinical judgment. The opportunity is not to automate clinical decisions — it is to help users understand what changed, what matters, and what action they can take next.
What This Changed
Research revealed that the Queue was acting as a manual planning layer for treatment readiness — and that most of that planning happened outside Lynx. That insight shifted the modernization direction from improving a high-traffic page to reframing the entire workflow around readiness.
Who is ready. What is blocked. What medication may be needed. Which vial configuration is recommended. Where human review is required. The system carries the calculation. Humans retain review, adjustment, and control.